EASy MAP Protocol
🎓 Train in the EASy module →A systematic approach to evaluating the hypotensive patient using point-of-care ultrasound
What is EASy MAP?
EASy MAP stands for Echocardiographic Assessment using Subxiphoid-Only — Mean Arterial Pressure.
It is a concise point-of-care ultrasound examination designed for immediate determination of cardiovascular and cardiorespiratory status in patients with hypotension (MAP < 65 mmHg). The full method — all six views, common pitfalls, and a 12-point cardiac image-quality scale — is published in the Journal of Visualized Experiments (2025).
Key Features
- Rapid acquisition -- Complete exam in under 5 minutes
- Single probe -- Uses only a phased array transducer
- Pattern recognition -- Identify hemodynamic phenotypes quickly
- Beginner-friendly -- 87% success rate after 1-day training
Patient Inclusion Criteria
Inclusion:
Mean Arterial Pressure (MAP) < 65 mmHg
Exclusions:
- Cardiac arrest with active compressions
- Unable to tolerate supine position
- Extreme obesity limiting image quality
The 6 EASy Views
Systematically acquire these six views using a phased array probe
Subcostal 4-Chamber View
Probe Position
- Place probe 2 cm inferior to xiphoid process
- Marker facing toward patient's left (3 o'clock)
- Use overhand grip
- Trap small skin fold for good contact
- Angle probe tail caudally toward patient's right
What to Assess
- Both ventricles (LV and RV)
- Both atria (LA and RA)
- Tricuspid and mitral valves
- Global LV and RV function
- Pericardium for effusion
Visualizes all 4 cardiac chambers
Subcostal IVC View
Probe Position
- Remove probe entirely from subcostal area
- Rotate marker to point cephalad (12 o'clock)
- Reposition at same location
- Angle beam slightly toward patient's left to identify aorta
What to Assess
- IVC Diameter: Normal 0.9-2.1 cm
- Collapsibility: >50% = collapsible
- Positively identify both IVC and aorta
- Look for hepatic vein draining into IVC
Critical: Always identify the aorta to avoid mistaking it for a non-collapsing IVC.
Assess preload and volume status
Upper Lung Views (Right & Left)
Probe Position
- 2nd intercostal space at midclavicular line
- Marker pointing cephalad (12 o'clock)
- Slide or tilt to minimize rib shadowing
- Repeat on both sides
What to Assess
- A-lines: Horizontal artifacts (normal/dry)
- B-lines: Vertical artifacts (wet/edema)
- Lung sliding: Normal pleural movement
A-lines vs B-lines assessment
Pleural Views (Right & Left)
Probe Position
- Right: Midaxillary line, same plane as subcostal view
- Left: Posterior axillary line, same horizontal plane
- Marker at 12 o'clock
- Identify liver/spleen, diaphragm, spine, and lung
What to Assess
- Pleural effusion or hemothorax
- Consolidation - spine sign, loss of curtain
- Diaphragm movement
Effusion and consolidation
Hemodynamic Phenotypes
Pattern recognition for rapid diagnosis and management
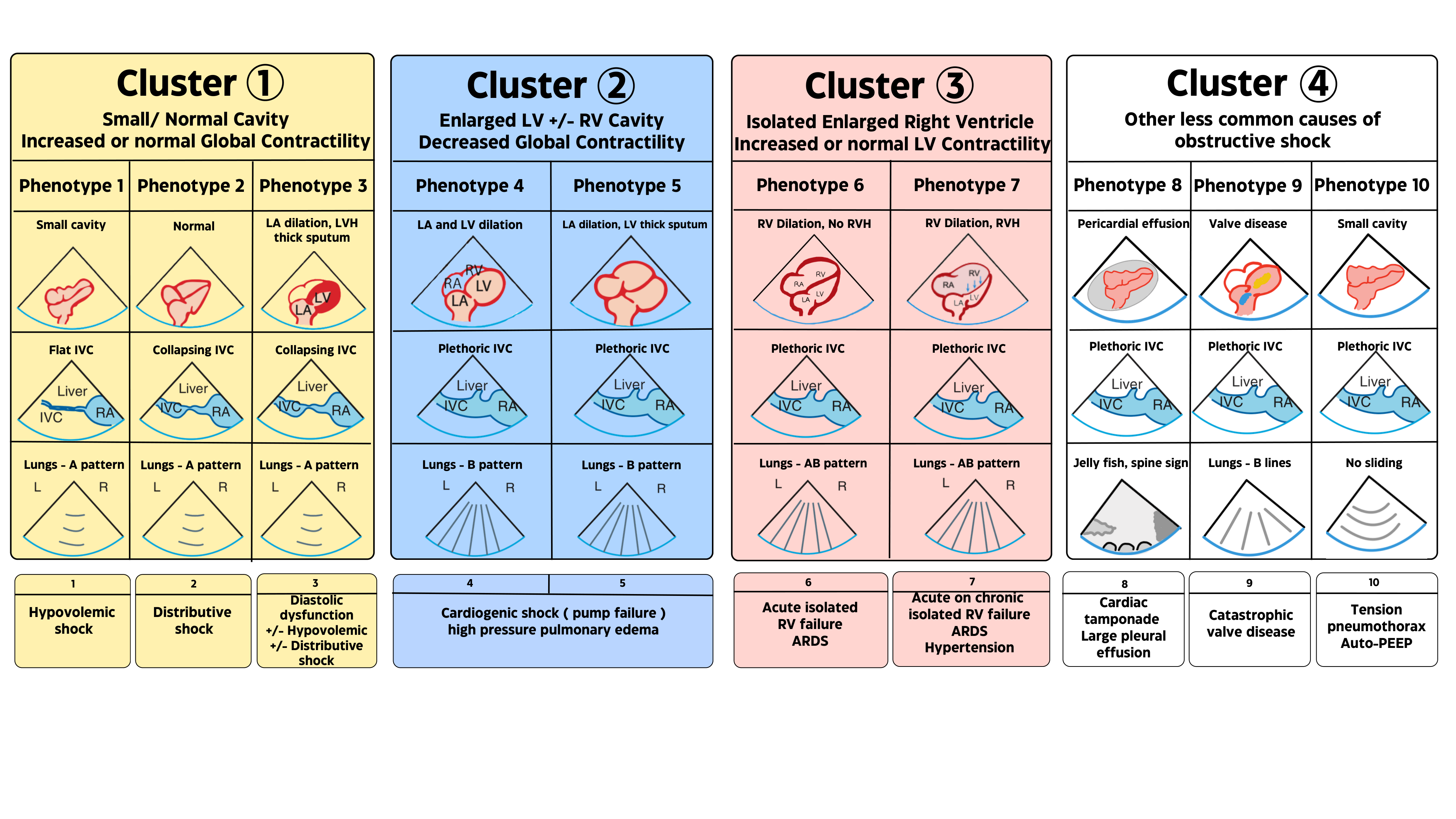
All 10 at a glance — cardiac · IVC · lung
| # | Cardiac | IVC | Lung | → Shock pattern |
|---|---|---|---|---|
| 1 | Small cavity | Flat | A-lines | Hypovolemic shock |
| 2 | Normal | Collapsing | A-lines | Distributive shock |
| 3 | LVH / thick septum | Collapsing | A-lines | Diastolic dysfunction |
| 4 | LA & LV dilation | Plethoric | B-lines | Cardiogenic shock (LV) |
| 5 | Bi-atrial / bi-ventricular dilation | Plethoric | B-lines | Biventricular failure |
| 6 | RV dilation, no RVH | Plethoric | A/B | Acute RV failure / ARDS |
| 7 | RV dilation + RVH | Plethoric | A/B | Acute-on-chronic RV failure |
| 8 | Pericardial effusion | Plethoric | Jellyfish / spine | Tamponade / large effusion |
| 9 | Valve disease | Plethoric | B-lines | Catastrophic valve disease |
| 10 | Small cavity | Plethoric | No sliding | Tension PTX / auto-PEEP |
Findings
- Small LV and RV cavities
- hyperdynamic function
- flat collapsing IVC
- A-lines on lung ultrasound
Consider: Hemorrhage, dehydration, third-spacing
Findings
- Normal/adequate LV and RV cavities
- hyperdynamic function
- normal or dilated IVC
- A-lines on lung ultrasound
Consider: Sepsis, anaphylaxis, neurogenic shock
Findings
- Thick-walled LV (concentric hypertrophy)
- small cavity appearance
- may be hypovolemic or distributive
Consider: Chronic hypertension, HFpEF
Findings
- Dilated LV
- severely reduced LV function
- plethoric IVC
- B-lines on lung ultrasound
Consider: AMI, cardiomyopathy, myocarditis
Findings
- Both LV and RV dilated
- globally reduced function
- plethoric IVC
- bilateral B-lines
Consider: End-stage cardiomyopathy, pulmonary edema
Findings
- RV > LV (RV/LV > 1)
- septal shift toward LV
- thin RV wall
- plethoric IVC
Consider: Massive PE, acute ARDS
Findings
- RV dilation with thick wall (>1 cm)
- RA enlargement
- septal flattening
- plethoric IVC
Consider: Pulmonary HTN, chronic PE, COPD
Findings
- Pericardial effusion >10mm
- chamber collapse (RA/RV diastolic)
- plethoric IVC
Findings
- Visible valve abnormality
- chamber dilation
- plethoric IVC
- B-lines pattern
Findings
- Small hyperdynamic heart
- plethoric IVC
- no lung sliding
- barcode sign on M-mode
Published methods
EASy MAP is a peer-reviewed, video-illustrated protocol. The methods paper demonstrates acquisition of all six views with a low-frequency phased-array transducer — subcostal cardiac and IVC for the cardiovascular assessment, supplemented by anterior upper-lung and posterolateral diaphragmatic pleural views for the respiratory assessment — along with common pitfalls and a 12-point scale for rating cardiac image quality.
Howell-Clark JR, Bronshteyn YS, Pustavoitau A, Convissar D, Bughrara N. Echocardiographic Assessment Using Subxiphoid-Only Examination for Hypotensive Patients. J Vis Exp. 2025;(218):e67531.Protocol Resources
Downloadable guides, checklists, and reference cards
Ready to learn EASy MAP?
Enroll in the fundamentals course or download the reference materials.